Tracheostomy

Procedure -
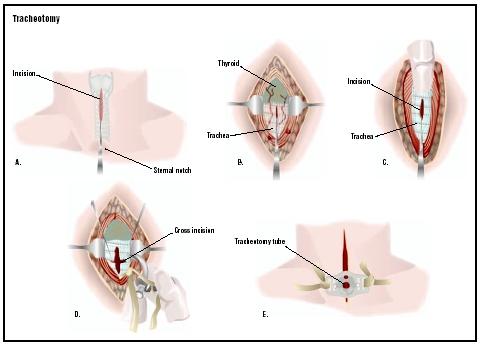
Position of the patient - The patient is lying supine with a sand bag below the shoulder so as to extend the neck and make the trachea prominent but in an already respiratory compromised patient, the patient becomes more uncomfortable with this posture.
The neck is painted with povidone iodine solution and sterile sheets placed. The area is infilterated with 2% lignocaine with adrenaline solution in a diamond shape fashion. The area is palpated and landmarks identified. The incision is placed two fingers above the suprasternal notch. Most of the times a transverse incision is given in a skin crease but in emergencies a vertical incision is of great help. The subcutaneous tissue is divided and muscles exposed. Great care is taken not to leave the midline otherwise one can land in complications. The fat which comes in the way can be safely removed to get a better exposure.The strap muscles are neatly separated in the midline with blunt dissection with a small artery forceps. Now the isthmus of thyroid comes in the way. This can be lifted up with a hook or clamped with long artery forceps, cut and transfixed with ligatures.The pretracheal tissue is gently dissected and trachea exposed and identified from tracheal rings. Small amount of local anaesthetic is injected in trachea to decrease the cough reflex after aspiration of air to confirm the position of needle.Now the trachea is incised between 2nd and 3rd tracheal or 3rd and 4th tracheal rings.A small piece of cartilage can be removed to facilitate the entry of tracheostomy tube but in children this is avoided. Now the tracheostomy tube is inserted and secured. The wound is closed with silk or prolene sutures.
posted by ENT at
9:04 PM
![]()
![]()

0 Comments:
Post a Comment
Subscribe to Post Comments [Atom]
<< Home