Tracheostomy

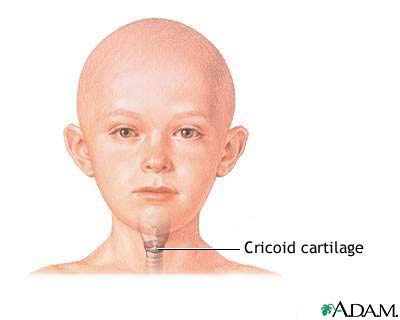


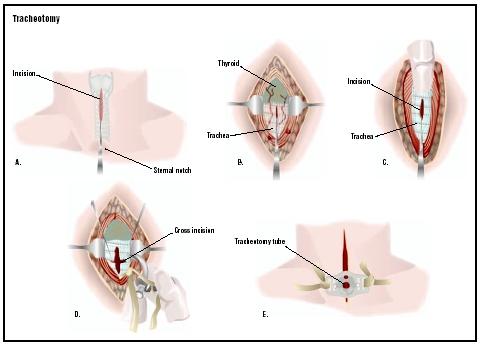
Landmarks for tracheostomy
- Cricoid cartilage - It is a circular cartilage below the thyroid cartilage and is the shape of a tyre. It is tne only cartilage in larynx and trachea which forms a complete ring and also it forms the widest ring and the most prominent one.
- Suprasternal notch - Make an incision two finger breadth above supra sternal notch.
- Strap muscles - these are separated vertically by blunt dissection.
- Isthmus of thyroid gland - If possible retract it upwards or if not put two clamps, cut and transfix it.
- Tracheal rings - palpate and confirm by aspirating with a syringe.
posted by ENT at
8:01 PM
0 Comments
![]()
![]()